How Peptide Vial Sizing Works for Research Accuracy
Understanding how peptide vial sizing works in research settings is one of those technical details that separates well-designed experiments from ones plagued by reproducibility problems. Many researchers treat vial size as a procurement afterthought, assuming any available format will serve equally well. It does not. The size of a peptide vial directly governs maximum reconstitution volume, achievable concentration, headspace integrity, and ultimately the precision with which doses can be measured using standard laboratory syringes. This article covers the mechanics of sizing selection, dosing calculations, storage implications, and syringe alignment in precise technical terms for biomedical researchers working with lyophilized research peptides.
Table of Contents
- Key takeaways
- Standard vial sizes and peptide load ranges
- Reconstitution volume, concentration, and dosing accuracy
- Vial handling, storage, and stability
- Syringe selection and dosing volume alignment
- My perspective on where researchers lose precision
- Supporting your research with verified peptide vials
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Vial size dictates reconstitution limits | The physical volume of a vial caps how much solvent you can add, directly setting the maximum achievable concentration. |
| Headspace is non-negotiable | Maintaining approximately 20% headspace prevents stopper damage and allows adequate peptide dissolution during reconstitution. |
| Concentration controls dose accuracy | Selecting the reconstitution volume strategically converts tiny microgram doses into measurable syringe units, reducing relative error. |
| Aliquoting extends peptide stability | Dividing reconstituted stock into single-use vials minimizes repeated freeze-thaw exposure and contamination risk. |
| Syringe selection must match vial concentration | Mismatched syringe size and peptide concentration is a leading source of dosing errors in laboratory settings. |
Standard vial sizes and peptide load ranges
Understanding peptide vials begins with the physical formats that suppliers actually produce. The industry-standard vial formats range from 2 mL to 10 mL, with the 3 mL borosilicate glass vial serving as the most widely used configuration across peptide suppliers. Each format corresponds to a practical range of peptide mass loading.
| Vial Size | Typical Peptide Load | Common Research Application |
|---|---|---|
| 2 mL | 1 to 5 mg | Short-duration studies, single-compound screening |
| 3 mL | 5 to 15 mg | Standard experimental runs, most catalog peptides |
| 5 mL | 5 to 30 mg | Multi-week studies requiring larger total amounts |
| 10 mL | 100 mg or more | Bulk research, multi-cohort experiments |
The rationale behind these formats is not arbitrary. Market demand and experimental duration shape the vial sizes vendors offer more than any single technical constraint. A typical 6 to 8 week experimental protocol drives demand for 5 mg to 10 mg vial configurations, which is why the 3 mL format dominates catalog offerings. Researchers working with peptides like TB-500, IGF-1 LR3, or Ipamorelin will encounter these formats consistently across qualified suppliers.

Beyond peptide mass, vial format also determines how much reconstitution solvent you can practically use. The maximum liquid volume in a 3 mL vial is approximately 2.5 mL, and a 2 mL vial accommodates between 1.5 and 2 mL of solvent. Exceeding these volumes risks stopper displacement, dissolution failure, and potential rubber particle contamination.
Key considerations when selecting a vial format:
- Match the vial size to the total peptide mass you ordered, not just the target dose
- Confirm the vial material is borosilicate glass, which resists leaching and maintains peptide integrity
- Never select a vial format where your required solvent volume exceeds 80% of total vial capacity
- Account for multi-week storage when sizing up, since a single large vial reconstituted early in a study may degrade before use
Reconstitution volume, concentration, and dosing accuracy
This is where understanding peptide vials becomes genuinely consequential for experimental design. The volume of bacteriostatic water or other approved solvent you add during reconstitution sets the peptide concentration, and that concentration determines the physical volume you must draw per dose.
The calculation is straightforward. Concentration (mg/mL) equals the total peptide mass in the vial divided by the volume of solvent added in milliliters. From there, the volume per dose equals the target dose divided by the concentration. The difficulty lies in choosing a concentration that makes your target dose measurable on a standard insulin syringe without introducing large relative errors.
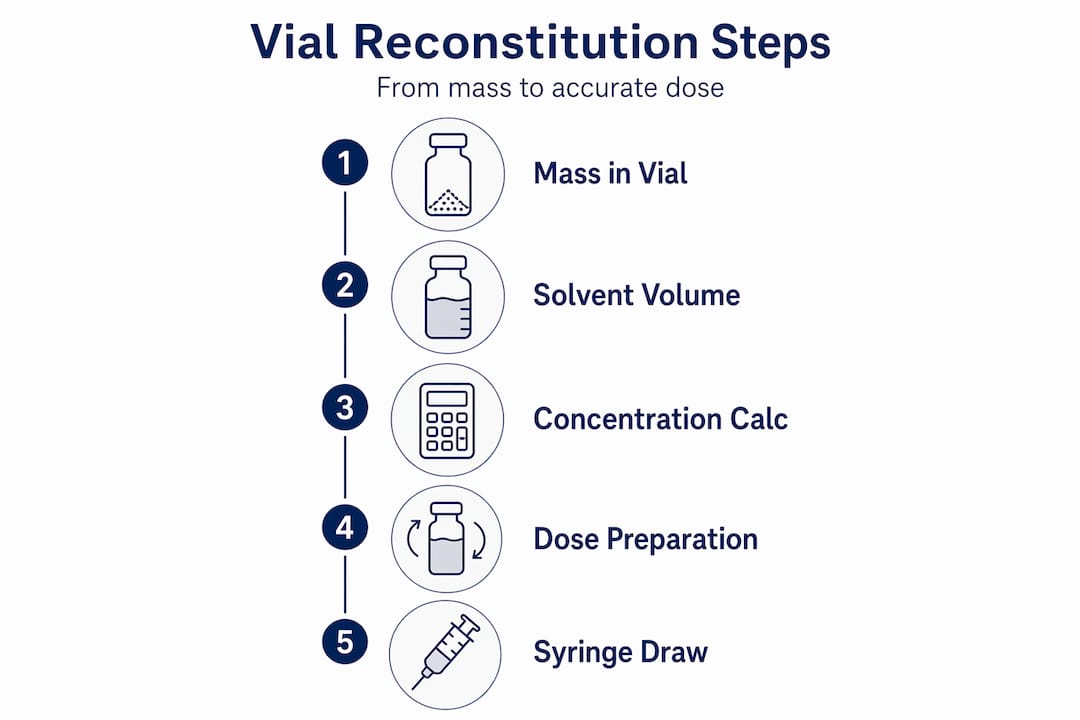
Consider a practical example. A 5 mg peptide vial reconstituted with 2 mL of bacteriostatic water yields a concentration of 2.5 mg/mL. A 250 mcg research dose at that concentration requires 0.1 mL, which corresponds to 10 units on a standard U-100 insulin syringe. That is a clear, unambiguous measurement. Now reconstitute the same 5 mg peptide in 0.5 mL instead, producing a 10 mg/mL concentration. The same 250 mcg dose now requires only 0.025 mL, or 2.5 units on the syringe. At that scale, a single graduation error doubles or halves your actual dose.
Working through the dose math before reconstitution is a protocol discipline many researchers skip. The recommended concentration range for most research applications falls between 1 and 5 mg/mL, which balances practical solvent volume with measurable syringe units.
- Determine the total peptide mass in the vial (from the batch COA)
- Identify the target dose in micrograms
- Select a reconstitution volume that places the resulting dose between 10 and 50 syringe units on a U-100 insulin syringe
- Verify that the selected reconstitution volume does not exceed 80% of vial capacity
- Document the final concentration on the vial label before storage
Insulin syringe unit markings derive from clinical insulin dosing conventions where 100 units equals 1 mL. This means syringe unit readings must always be converted back to volume and then to peptide mass to confirm the actual dose delivered. Researchers who skip this conversion step introduce dosing errors that can exceed 10-fold, which compromises dose measurement reliability severely enough to invalidate experimental results.
Pro Tip: Before reconstituting any vial, write out the full dose math on paper or in your lab notebook: total mass, solvent volume, resulting concentration, dose volume in mL, and dose volume in syringe units. Cross-check by working the calculation in reverse. This takes under two minutes and catches unit conversion errors before they become an experimental variable.
Vial handling, storage, and stability
How peptide vial sizes affect results extends beyond the bench reconstitution step. Storage conditions and vial handling practices interact directly with physical vial dimensions and the amount of peptide mass per container.
Lyophilized peptide vials stored at approximately -20°C remain stable for 18 to 24 months when unopened. Once reconstituted, the working solution stored at 2 to 8°C remains usable for approximately 30 days under standard conditions, though sensitive sequences may require use within 14 days. These timelines have direct implications for how you select vial sizing relative to your experimental schedule.
Headspace inside the vial is a structural requirement, not a suggestion. Insufficient headspace during reconstitution impairs dissolution and risks stopper damage, which can introduce rubber particulate contamination into the peptide solution. Maintaining approximately 20% headspace above the liquid surface resolves both concerns.
Best practices for storage and handling:
- Store lyophilized vials at -20°C in a dedicated freezer away from repeated door-opening cycles
- After reconstitution, transfer to 2 to 8°C refrigerated storage immediately and label with the reconstitution date
- Temperature cycling and freeze-thaw of reconstituted solutions causes irreversible peptide degradation. Lyophilized peptides tolerate freeze-thaw cycles; aqueous solutions do not
- Aliquot reconstituted stock into single-use volumes immediately after reconstitution to avoid repeated needle penetration of the same vial
The aliquoting practice deserves particular emphasis. Aliquoting reconstituted peptide solutions into single-use vials reduces contamination and degradation risk compared to maintaining one large multi-use vial throughout an extended experiment. Many labs skip this step because it adds preparation time, but failure to aliquot risks progressive loss of peptide integrity across a multi-week study. Draw the full reconstituted volume into separate vials, freeze those not needed immediately, and thaw individual aliquots only as needed.
Pro Tip: Label each aliquot vial with the peptide name, batch number, concentration, aliquot date, and estimated volume. A printed label or clear permanent marker notation takes seconds per vial and creates a traceable record that supports data integrity across the entire experimental run.
Syringe selection and dosing volume alignment
The final variable in how peptide vial sizing works in research settings is the physical syringe used to measure doses. Vial format and reconstitution volume selection are only useful if the resulting concentration aligns with the measurement resolution of the syringe format you plan to use.
| Syringe Size | Graduation Increment | Optimal Dose Volume Range |
|---|---|---|
| 0.3 mL (U-100) | 0.5 units | 3 to 30 units (0.03 to 0.3 mL) |
| 0.5 mL (U-100) | 1 unit | 5 to 50 units (0.05 to 0.5 mL) |
| 1.0 mL (U-100) | 2 units | 10 to 100 units (0.10 to 1.0 mL) |
The 0.3 mL insulin syringe with half-unit graduation offers the highest measurement precision for small research doses. Measuring a dose of fewer than 3 units on a 1.0 mL syringe introduces a relative error that can reach 30 to 50% of the target volume, depending on graduation alignment. That level of imprecision is incompatible with controlled experimental design.
Aligning your reconstitution math with syringe selection involves a few practical steps:
- Calculate your target dose volume before selecting the reconstitution volume
- Verify that the resulting dose volume falls between 10% and 80% of your chosen syringe capacity
- Use the smallest syringe that accommodates the full dose volume without drawing past the final graduation
- For doses below 50 mcg, the 0.3 mL syringe with half-unit markings is the correct tool regardless of reconstitution volume
- If your calculated dose falls below 5 units on any available syringe, increase the reconstitution volume to dilute the concentration and bring the dose volume into a more precise measurement range
See the peptide assay lab setup guide for step-by-step methods for calculating correct peptide quantities before reconstitution. Proper pre-reconstitution calculation is part of any defensible experimental protocol.
My perspective on where researchers lose precision
In my experience working with research-grade peptide documentation and laboratory protocols across a wide range of experimental designs, the most common source of dosing error is not a miscalculation. It is the assumption that the reconstitution volume written in a general protocol guide matches the vial size and peptide mass a researcher actually has in hand.
I have reviewed protocols where researchers applied a published reconstitution volume directly to a vial containing a different peptide mass than the original source specified. The concentration was wrong before a single dose was measured. The fix is verification. Check the batch COA for confirmed peptide mass, confirm it against the vial label, and then run your own concentration math from that confirmed figure.
My preference is always for smaller aliquot vials and a more dilute working concentration over concentrated stock solutions. The minor additional preparation time is a reasonable trade for consistent, measurable dose volumes and reduced degradation exposure. Convenience and precision rarely favor the same choice. Choose precision.
For the reconstitution lab protocol specifics, documented calculation steps are available to support verification before you commit to a reconstitution scheme.
— Vertex
Supporting your research with verified peptide vials
Vertexpeptideslab provides research-grade peptide vials in standardized formats, each supported by batch-specific Certificates of Analysis confirming purity greater than 99% through third-party HPLC and LC-MS verification. Every vial in the catalog includes documented peptide mass, enabling the precise concentration calculations described throughout this article. Researchers can explore the research catalog to review available vial configurations, access COA documentation, and request custom synthesis options suited to specific experimental requirements. All compounds are supplied for laboratory research use only. Not for human or veterinary use.
FAQ
What are the standard peptide vial sizes in research?
Standard vial sizes range from 2 mL to 10 mL, with the 3 mL borosilicate glass vial serving as the most common format. Peptide loads typically range from 1 to 5 mg in 2 mL vials and up to 100 mg or more in 10 mL configurations.
How does reconstitution volume affect peptide concentration?
The concentration equals total peptide mass divided by the volume of solvent added. Adding 2 mL to a 5 mg vial yields 2.5 mg/mL. Changing the reconstitution volume directly changes the dose volume required per measurement, which affects syringe precision.
Why does headspace matter in peptide vials?
Headspace of approximately 20% of total vial volume is required to allow adequate mixing during reconstitution and to prevent stopper displacement. Insufficient headspace risks rubber particle contamination and incomplete peptide dissolution.
How long do reconstituted peptide solutions remain stable?
Reconstituted peptide solutions stored at 2 to 8°C remain stable for approximately 30 days. Sensitive peptide sequences may require use within 14 days. Lyophilized unopened vials stored at -20°C remain stable for 18 to 24 months.
Which syringe size provides the most accurate peptide dosing?
The 0.3 mL U-100 insulin syringe with half-unit graduations offers the highest precision for small research doses. Doses measured below 3 units on a 1.0 mL syringe carry unacceptably high relative measurement error for controlled experimental use.