How the Peptide Therapeutics Pipeline Works in 2026
The peptide therapeutics pipeline is defined as a multi-stage drug development process that transforms computationally designed or naturally derived peptide sequences into scalable pharmaceutical candidates through iterative optimization, regulatory validation, and manufacturing scale-up. Understanding peptide therapeutics requires recognizing that this pipeline is not linear. It operates as a feedback loop in which computational predictions, experimental results, and developability data continuously inform one another. Peptides now target approximately 85% of previously “undruggable” human protein targets, a figure that explains the accelerating investment in this class of molecules. The stages covered here span AI-driven discovery, chemical modification, nonclinical safety assessment, clinical trials, and cGMP manufacturing compliance.
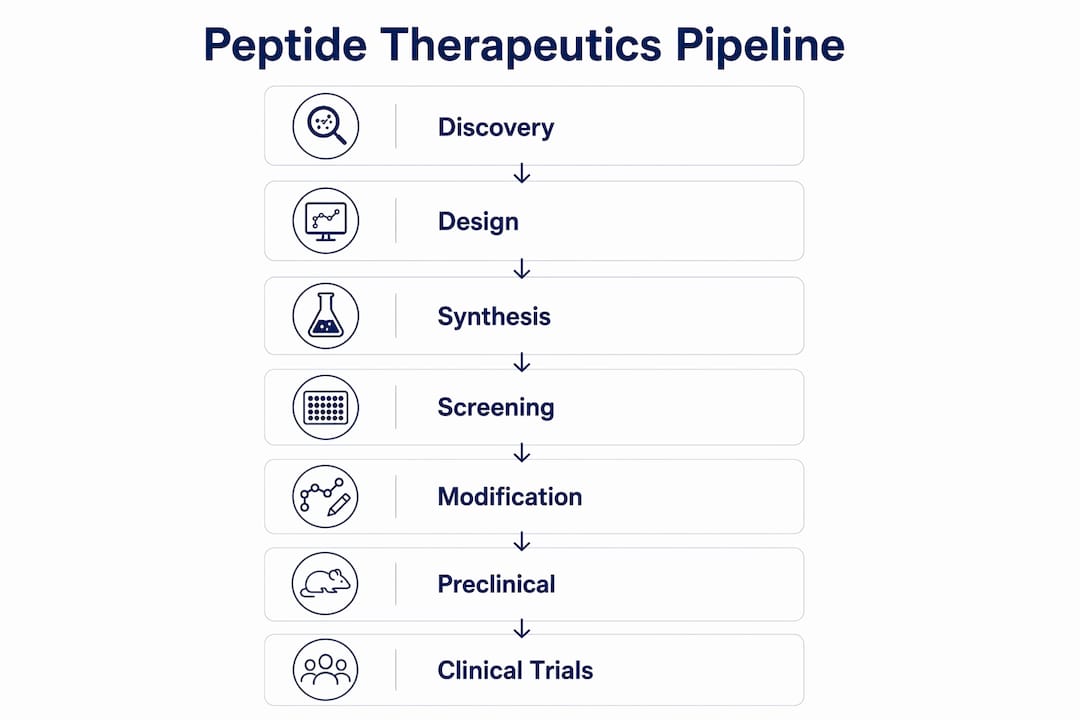
How the peptide therapeutics pipeline works: from discovery to candidate
The peptide therapy development process begins with target identification and sequence generation, where computational tools now do the heavy lifting. Machine learning models, including convolutional neural networks (CNNs), recurrent neural networks (RNNs), and graph neural networks (GNNs), analyze sequence-structure-activity relationships to predict bioactivity, proteolytic stability, and toxicity risk before a single synthesis run occurs. This iterative design-test-refine approach has compressed early discovery timelines significantly, though it has also exposed a persistent challenge: many computationally designed peptides fail at the developability stage due to aggregation, poor solubility, or off-target binding.
Generative AI models now enable de novo peptide design incorporating non-canonical amino acid residues, expanding the chemical space available to researchers well beyond the 20 standard residues. AstraZeneca’s peptide discovery program, for example, uses automation and AI-guided high-throughput screening to manage the high attrition inherent in early candidate generation. The output of this stage is not a single lead compound but a ranked library of candidates, each scored against multiple predicted properties simultaneously.

The critical limitation here is that in silico predictions remain probabilistic. Aggregation propensity, membrane permeability, and immunogenicity are notoriously difficult to model with precision, which is why computational design requires subsequent experimental validation at every iteration. Researchers who treat AI outputs as final answers rather than starting hypotheses consistently encounter higher attrition rates downstream.
Key capabilities driving early-stage peptide candidate optimization include:
- Sequence generation: Generative models propose novel sequences with predicted target affinity and selectivity profiles.
- Property prediction: ML models screen for solubility, stability, and toxicity flags before synthesis.
- Structural analysis: GNNs model peptide-receptor interactions at atomic resolution to guide affinity optimization.
- Iterative feedback: Experimental assay results are fed back into models to retrain and improve prediction accuracy.
- Non-canonical residue incorporation: Generative models propose D-amino acids, beta-amino acids, and peptidomimetic scaffolds to improve metabolic stability.
Pro Tip: Run developability screening, including aggregation and solubility assays, immediately after the first synthesis round rather than after full lead optimization. Catching these failures early prevents significant expenditure on candidates that will not survive formulation.
What chemical modifications do to peptide drug candidates
Peptide drug development success depends on overcoming three core pharmacokinetic liabilities: rapid enzymatic degradation, poor membrane permeability, and short plasma half-life. Chemical modification strategies address each of these directly, and the choice of modification determines not only the pharmacokinetic profile but also the manufacturability and immunogenicity risk of the final candidate.
The most widely applied modifications in current peptide pipeline stages are cyclization, PEGylation, lipidation, and hydrocarbon stapling. Each carries a distinct trade-off profile that researchers must evaluate against their specific target and delivery requirements.
| Modification | Primary benefit | Key trade-off |
|---|---|---|
| Cyclization | Proteolytic resistance, conformational rigidity | Reduced synthetic flexibility, higher production cost |
| PEGylation | Extended half-life, reduced renal clearance | Potential immunogenicity, reduced receptor binding affinity |
| Lipidation | Membrane association, albumin binding for half-life extension | Aggregation risk, formulation complexity |
| Hydrocarbon stapling | Alpha-helix stabilization, cell penetration | Synthesis complexity, limited commercial scale-up precedent |
Cell-penetrating peptides (CPPs) represent a formulation-level strategy rather than a covalent modification. CPPs such as TAT-derived sequences and penetratin facilitate intracellular delivery of otherwise membrane-impermeant cargo, expanding the target scope of peptide therapeutics to include intracellular protein-protein interactions. Researchers working on peptide formulation development will recognize that CPP conjugation introduces its own set of stability and immunogenicity variables that require systematic characterization.
Manufacturability is a constraint that chemical modification decisions must account for from the outset. A stapled peptide that demonstrates excellent in vitro activity but requires a 40-step synthesis is unlikely to survive the transition to cGMP production at scale. Early-stage developability screening, which evaluates aggregation propensity, solubility under physiological conditions, and compatibility with standard solid-phase peptide synthesis (SPPS) platforms, functions as the gatekeeping step that separates viable candidates from those that will fail at scale-up.
Pro Tip: When evaluating lipidation strategies, assess albumin binding affinity alongside half-life data. Strong albumin binding can mask immunogenicity risks that only emerge under high-dose or repeat-administration conditions in preclinical models.
What nonclinical safety requirements look like for peptide IND submissions
Regulatory expectations for peptide therapeutics before first-in-human (FIH) trials are defined primarily by FDA guidance and ICH harmonized guidelines. The nonclinical safety package must include GLP-compliant toxicology and pharmacology studies conducted in at least one rodent and one non-rodent species, with the objective of establishing safety margins and the maximum tolerated dose (MTD). SureNano Science’s 2026 IND-enabling program for GLP-GEP-44 illustrates this requirement directly: GLP toxicology studies in both rodent and non-rodent species were initiated to define dosing strategies and support regulatory submission readiness.
The genotoxicity component of the nonclinical package follows the ICH S2(R1) guideline, which specifies a standard battery of in vitro and in vivo assays. The ICH-aligned genotoxicity battery typically includes a bacterial reverse mutation assay (Ames test), an in vitro chromosomal aberration or micronucleus assay, and an in vivo rodent micronucleus or comet assay. Weight-of-evidence interpretation is applied when results across assays are discordant, which is common for peptides with novel non-canonical residues.
The nonclinical safety package for a peptide IND submission must address the following elements in sequence:
- Pharmacology studies: Primary pharmacodynamic studies establishing mechanism of action and target engagement, plus secondary pharmacodynamic studies assessing off-target receptor binding.
- Safety pharmacology: Core battery studies evaluating cardiovascular (hERG channel), central nervous system, and respiratory function per ICH S7A/S7B.
- Repeat-dose toxicology: GLP-compliant studies in rodent and non-rodent species at multiple dose levels to establish the no-observed-adverse-effect level (NOAEL) and MTD.
- Genotoxicity: ICH S2(R1)-aligned battery including Ames test, in vitro micronucleus assay, and in vivo follow-up where indicated.
- Immunogenicity assessment: Anti-drug antibody (ADA) analysis to characterize immune response potential, particularly relevant for peptides with non-canonical residues or novel scaffolds.
- Bioanalytical method validation: Validated assays for quantifying the peptide and its metabolites in biological matrices, required for toxicokinetic data supporting dose selection.
Impurity profiling deserves specific attention in peptide regulatory dossiers. Unlike small molecules, synthetic peptides carry sequence-related impurities (deletion sequences, truncation products) and process-related impurities (protecting group remnants, coupling reagents) that must be characterized and controlled. Researchers evaluating peptide stability testing protocols will find that the analytical methods developed for stability studies often form the foundation for the bioanalytical validation package submitted with the IND.
How clinical phases and manufacturing compliance shape the peptide pipeline
The peptide pipeline stages from preclinical through regulatory review follow a defined sequence, though timelines vary considerably based on indication, formulation complexity, and regulatory pathway. The current peptide clinical pipeline includes over 300 active preclinical programs, with Phase III trials averaging approximately 3.5 years in duration. That figure reflects the complexity of demonstrating efficacy and safety in adequately powered patient populations for a molecule class that often requires specialized delivery systems.
Phase I trials for peptides focus on safety, tolerability, and pharmacokinetic characterization in healthy volunteers or, for oncology indications, in patients. Phase II establishes proof-of-concept efficacy and dose-range finding. Phase III trials are the most resource-intensive stage, requiring large patient cohorts and often encountering formulation-related challenges that were not apparent at smaller scale. Integrated CMC-to-FIH workflows have demonstrated that parallel development workstreams covering API process development, drug product formulation, and analytical method validation can compress timelines to approximately 11 months from program initiation to Phase 1 entry.
Manufacturing compliance for peptide therapeutics operates under 21 CFR Part 211, which received significant amendments in 2026. The cGMP modernization updates introduce explicit expectations for data integrity, computerized system controls aligned with 21 CFR Part 11, and continuous process verification (CPV) as a standard requirement rather than an optional quality tool. These changes have direct implications for how manufacturers document batch records, manage electronic audit trails, and validate analytical instruments used in release testing.
Key manufacturing compliance requirements under the 2026 cGMP framework include:
- Data integrity controls: All electronic records must meet ALCOA+ principles (attributable, legible, contemporaneous, original, accurate, plus complete, consistent, enduring, and available).
- Computerized system validation: Systems used in manufacturing and quality control must be validated per 21 CFR Part 11 and current GAMP 5 guidance.
- Continuous process verification: Ongoing statistical monitoring of critical process parameters and critical quality attributes throughout commercial production.
- Audit trail requirements: Immutable, time-stamped records of all data entries, modifications, and deletions in electronic batch records.
Researchers evaluating peptide manufacturing quality benchmarks will find that the 2026 amendments raise the documentation bar considerably, particularly for facilities transitioning from paper-based to electronic quality management systems.
Key takeaways
The peptide therapeutics pipeline succeeds when AI-driven discovery, chemical modification, ICH-aligned safety assessment, and cGMP-compliant manufacturing are executed as integrated, iterative workstreams rather than sequential handoffs.
| Point | Details |
|---|---|
| Pipeline is iterative, not linear | Computational predictions require experimental validation at every stage, creating continuous feedback loops. |
| Chemical modification is a strategic decision | Cyclization, PEGylation, lipidation, and stapling each carry distinct manufacturability and immunogenicity trade-offs. |
| Nonclinical package is regulatory-defined | GLP toxicology in rodent and non-rodent species, plus ICH S2(R1) genotoxicity, are non-negotiable for IND submission. |
| Integrated CMC workflows compress timelines | Parallel API, formulation, and analytical workstreams can achieve Phase 1 entry in approximately 11 months. |
| 2026 cGMP amendments raise documentation standards | Data integrity, computerized system validation, and continuous process verification are now explicit FDA expectations. |
What we have observed about the direction of peptide pipeline development
From our position working with biomedical researchers who require verified, high-purity research peptides, we have observed a consistent pattern: the programs that advance most efficiently are those that treat developability screening as a first-class scientific activity rather than an administrative checkpoint. The tendency to prioritize pharmacological potency data over solubility, aggregation, and manufacturability profiles is the single most common source of late-stage attrition we see reflected in the research literature and in the questions researchers bring to us.
The integration of AI prediction with wet-lab experimental cycles is genuinely changing the pace of early discovery. What concerns us, however, is the assumption that computational confidence scores translate directly into developability confidence. They do not. A peptide with a predicted high binding affinity and a predicted low aggregation score still requires physical characterization under the exact buffer, temperature, and concentration conditions relevant to its intended formulation. We have seen programs lose months by skipping this step.
The regulatory environment in 2026 is more demanding than it was five years ago, particularly around data integrity and electronic record management. Researchers building IND packages need to account for this not just in their manufacturing documentation but in how they manage analytical data from preclinical studies. The quality of documentation at the research stage sets the precedent for the quality of documentation at the regulatory stage.
The expansion of peptide target scope to include intracellular protein-protein interactions, driven by CPP conjugation and stapled peptide formats, is the development we find most scientifically significant for the next decade of pipeline activity. The role of peptide biomarkers in identifying and validating these targets will become increasingly central to early-stage program design.
— Vertex
Supporting your peptide research with verified materials and documentation
Vertexpeptideslab provides research-grade synthetic peptides with documented purity greater than 99%, verified through third-party HPLC and LC-MS analysis. Every batch in the Vertexpeptideslab catalog is accompanied by a Certificate of Analysis (COA) that records identity confirmation, purity data, and batch-specific quality parameters. For researchers working within the peptide pipeline stages described in this article, access to analytically characterized reference materials is a prerequisite for generating reproducible preclinical data. Explore the research peptide catalog to review available compounds, COA documentation, and custom synthesis options. For laboratory research use only. Not for human or veterinary use.
FAQ
What are peptide therapeutics in drug development?
Peptide therapeutics are pharmaceutical candidates composed of short amino acid chains, typically 2 to 50 residues, designed to modulate specific biological targets with high selectivity. They occupy a chemical space between small molecules and biologics, offering tunability that makes them particularly suited to targeting protein-protein interactions.
How long does the peptide pipeline take from discovery to Phase 1?
Integrated CMC-to-FIH workflows can compress timelines to approximately 11 months from program initiation to Phase 1 entry when API development, formulation, and analytical validation proceed in parallel. Standard sequential programs typically require 18 to 36 months for the same transition.
What is the most common reason peptide candidates fail in development?
Developability failures, including poor solubility, aggregation propensity, and proteolytic instability, account for the majority of attrition in peptide pipelines. These issues are often identified late when developability screening is not integrated into early-stage candidate selection.
What regulatory guidelines govern peptide nonclinical safety studies?
FDA IND requirements and ICH guidelines, specifically ICH S7A, S7B, and S2(R1), define the nonclinical safety package for peptide therapeutics. GLP-compliant toxicology studies in rodent and non-rodent species are required before first-in-human dosing.
How do the 2026 cGMP amendments affect peptide manufacturing?
The 2026 amendments to 21 CFR Part 211 introduce explicit requirements for data integrity controls, computerized system validation aligned with 21 CFR Part 11, and continuous process verification as standard manufacturing practice for peptide drug products.